- OrthoThrive
- Posts
- History of Amercian Orthodontics 3/1
History of Amercian Orthodontics 3/1
From Wartime Ingenuity to a Transatlantic Conversation in Orthodontics
Borris Upton
August 10, 2025
A Field Comes of Age
By the early 1930s, American orthodontics had a clear identity. Edward H. Angle’s classification system had become the profession’s common diagnostic language, and his Edgewise Appliance set the technical benchmark. In the decades that followed, the field grew beyond his influence, shaped by economic hardship, wartime necessity, and an ongoing exchange of ideas with Europe.
Material Advances in a Time of Scarcity
The Great Depression and World War II tested dentistry’s resourcefulness. Gold — long the material of choice for archwires — became scarce and prohibitively expensive. Orthodontists began turning to stainless steel, which had been available since the 1920s but was initially viewed with skepticism. Many worried it lacked the springiness and corrosion resistance of noble metals.
By the late 1930s, clinical results told a different story. Stainless steel archwires offered durability, lighter forces, and easier manipulation. They retained shape better than gold and significantly reduced patient discomfort. An example often cited in mid-century orthodontic literature was the ability to open a constricted maxillary arch in weeks rather than months. The shift also lowered treatment costs, enabling more middle-class families to seek care for their children.
Wartime Influence on Technique
World War II’s dental demands went far beyond fillings and extractions. Military dental units treated soldiers with maxillofacial injuries from shrapnel, blast impacts, and fractures. Orthodontists, sometimes embedded with surgical teams, applied their mechanical skills to splinting jaws, stabilizing occlusion, and aiding post-traumatic reconstruction.
Functional appliances were useful in certain cases. In resource-limited wartime clinics, appliances like modified monoblocks could help restore jaw function when full fixed treatment wasn’t feasible. Case reports from field hospitals show examples of monoblocks fabricated quickly from vulcanite to assist soldiers with mandibular fractures in regaining normal chewing function.
The Tweed Revolution
In the 1940s, Charles H. Tweed challenged one of Angle’s central doctrines: non-extraction therapy. After seeing many of his own non-extraction cases relapse, Tweed began advocating for strategic extractions, especially premolars, to achieve more stable and harmonious facial profiles.

Leveling and alignment — A series of round archwires was used by Tweed.
In: Vaden, James L. A century of the edgewise appliance.
His Tweed Technique refined the Edgewise method by controlling incisor angulation with precise wire bending. The “diagnostic facial triangle” — an evaluation of the relationship between the lower incisor, chin, and facial profile — became a standard in orthodontic education. In one well-documented case, Tweed treated a severely protrusive Class II malocclusion by extracting upper first premolars, retracting anterior teeth, and improving lip competence — a result that held decades later.

Fully banded standard edgewise appliances with space-closing loops in the upper and lower archwires in situ. https://pocketdentistry.com/contemporary-fixed-appliances/
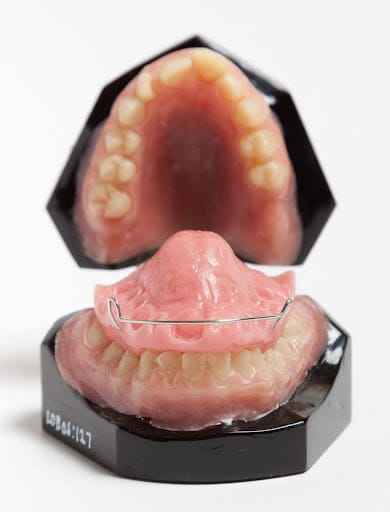
Tweed asked on proper Retention stated: “As a rule, in my office, retention varies from none at all to as much as 4 or 5 years. As a general rule, when active treatment has been completed, the retaining devices of my choice are two Hawley retainers, a maxillary and a mandibular.”
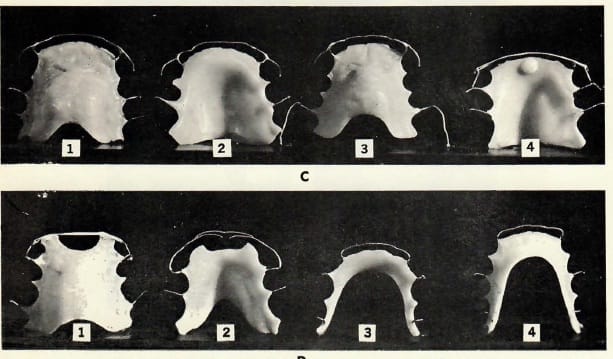
Fig. 2 Examples of retainers used with the Tweed Technique. (From Tweed: Clinical Orthodontics, The C.V. Mosby Co., St. Louis, MO. 1966). In: Brandt, Sidney. JPO Interviews Dr. Charles H. Tweed, Part 3
Postwar Growth and Standardization
After 1945, American orthodontics expanded rapidly. Returning veterans used the G.I. Bill to enter dental and orthodontic programs. Membership in the American Association of Orthodontists surged. Appliance manufacturing embraced mass production — prefabricated bands, standard-sized brackets, and preformed archwires shortened chairside time and improved consistency.
An average postwar orthodontic office might now treat dozens of patients simultaneously with nearly identical bracket systems, a level of standardization unthinkable in Angle’s day.
Transatlantic Exchange in Appliance Design
If the 1930–1960 period was about refinement in the U.S., it was also about borrowing, adapting, and improving ideas from Europe — particularly in the field of functional appliances. These devices, designed to influence jaw growth and muscle function, had deep European roots.
European Functional Appliance Legacy
The mid-century transatlantic exchange brought functional appliances from European innovators into American practice. These designs aimed to guide jaw growth and muscle function rather than move teeth alone.
Pierre Robin and the Monoblock
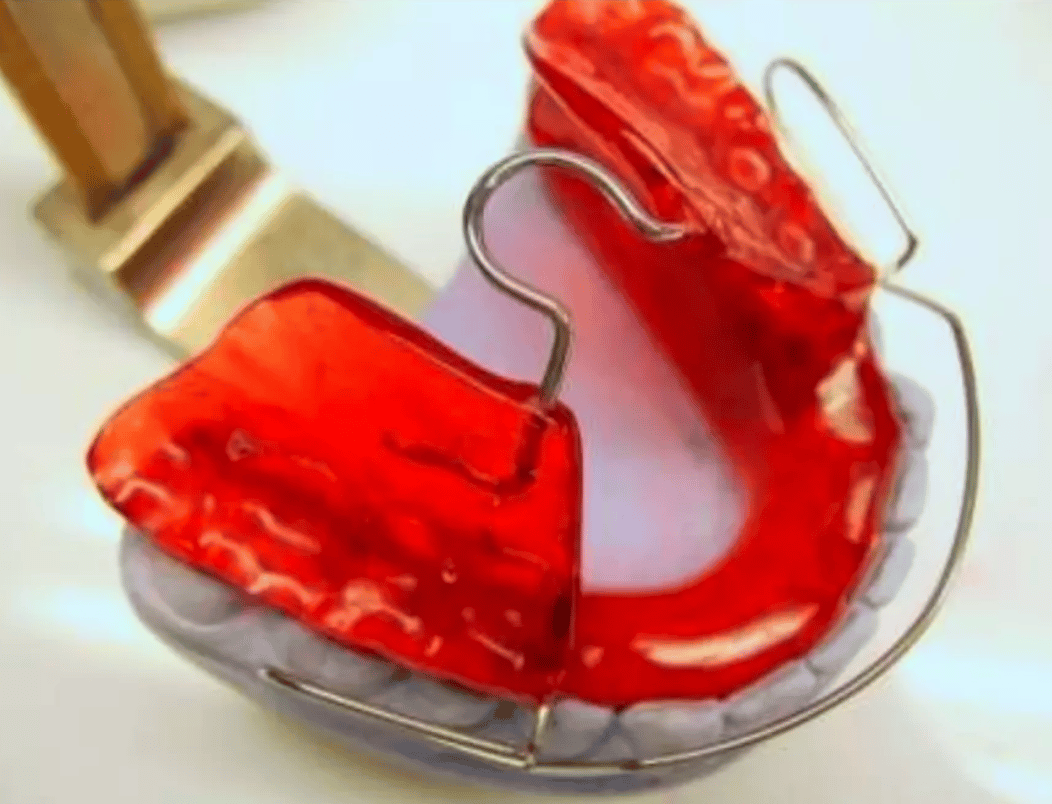
In France in the early 1900s, physician Pierre Robin sought to help children with micrognathia (undersized lower jaws) and airway problems. His Monoblock appliance, a single-piece acrylic block holding the upper and lower jaws in a forward position, was originally intended to prevent airway collapse. Over time, it became a tool for guiding mandibular growth in young patients.
Andresen’s Activator
In the 1920s, Viggo Andresen, a Danish orthodontist, refined Robin’s concept into the Activator. While Robin’s device was primarily for airway and jaw posture, Andresen created a functional orthopedic tool that could influence dental arches and skeletal relationships during growth. Working with German collaborator Karl Häupl, Andresen refined the appliance into a systematic functional jaw orthopaedic treatment.
Andresen Activator. In: British Orthodontic Society. Functional-Appliances
The Activator was acrylic, covering both dental arches, and worn mostly at night. It positioned the mandible forward in Class II patients, stimulating adaptive changes in muscle patterns and bone growth. By the 1930s, it was in use throughout Scandinavia and Germany — and eventually crossed into American hands in the postwar period.
Further Developments: From Korkhaus to the Bionator
Subsequent decades saw refinements aimed at improving comfort, speech, and versatility:
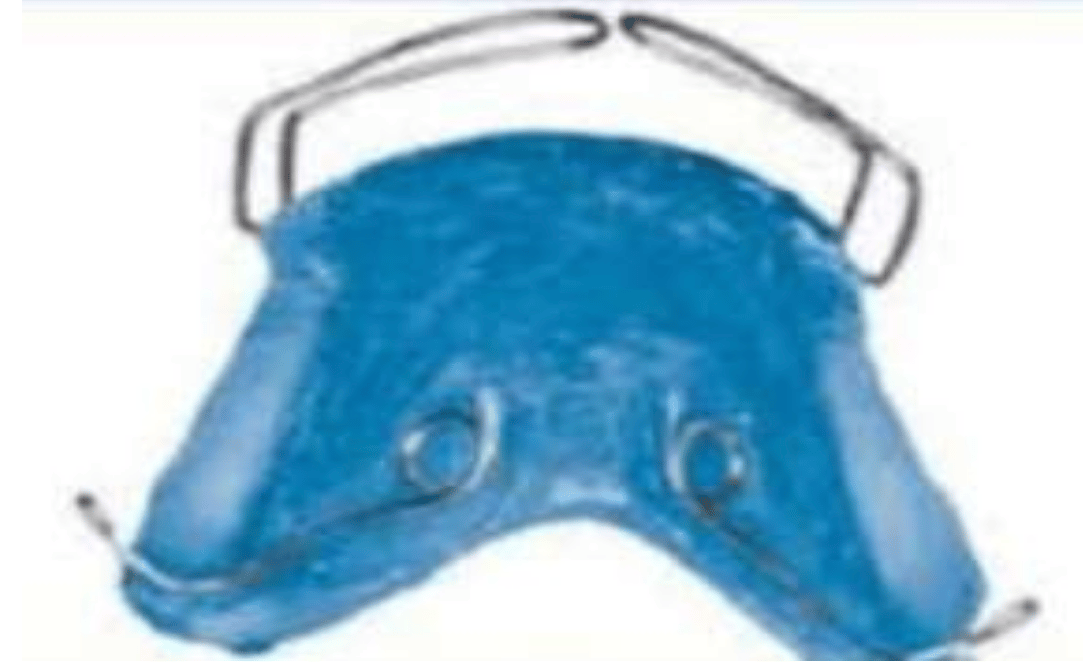
Korkhaus Activator (Germany, 1930s) — Incorporated labial bows and screws for tooth movement alongside jaw guidance.
Wilhelm Balters’ Bionator (Germany, 1950s) — Lighter and less bulky, allowing better speech during wear. Widely adopted in both Europe and South America.
Bionator appliance. In: Bionator
Bionator appliance in situ. In: Treatment effects of the Jasper Jumper and the Bionator associated with fixed appliances. Neves et al.
Hänschen and Harvold (Norway, 1960s) — Integrated asymmetric adjustments and vertical control for complex growth patterns.
These developments kept the same core principle: skeletal correction through mandibular posturing and neuromuscular adaptation.
Harvold/Woodside activator. In: The activator and its modification - A review.
The Crozat Appliance — A Parallel American Path
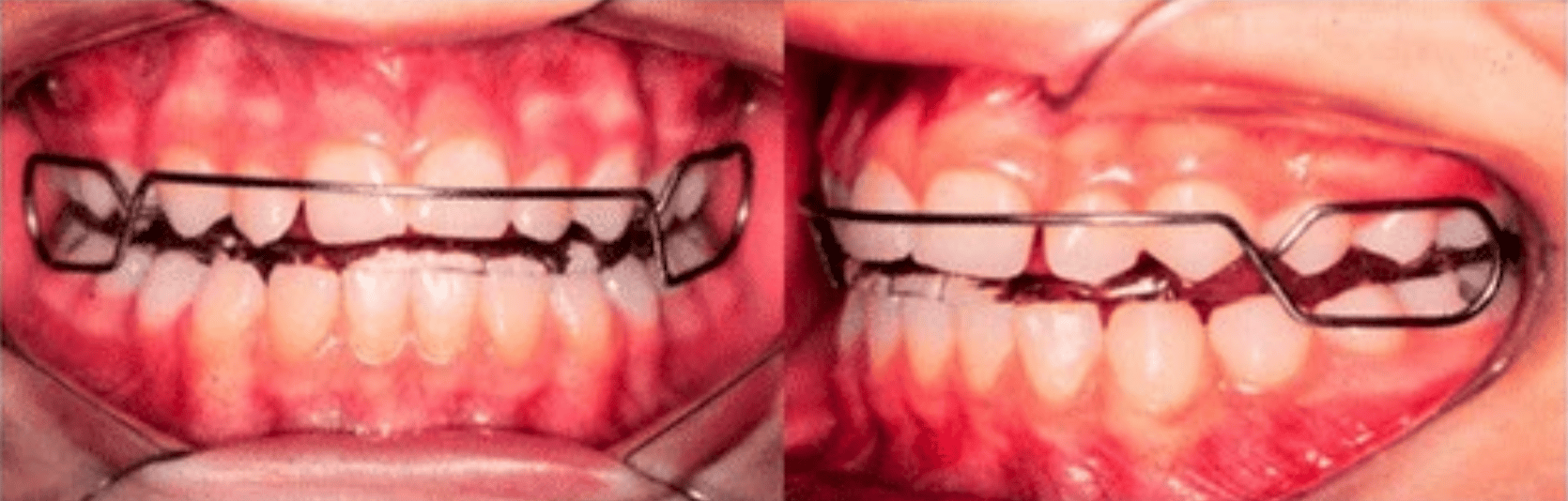
While Europe developed acrylic-block appliances, Dr. George B. Crozat in New Orleans took a different approach. In 1919, he introduced his Crozat Appliance, a delicate, removable lightwire device made of precious metals. It used finger springs and clasps to expand arches and move molars distally, often without the bulk of acrylic.
Crozat’s philosophy was distinct:
Gentle forces for skeletal development rather than aggressive expansion.
Arch coordination without routine premolar extractions.
A focus on molar and premolar expansion guided by Pont’s Index.
The appliance gained followers, especially among general dentists, and evolved into later designs made from non-corrosive alloys. Its design principles became a direct ancestor to the ALF (Advanced Lightwire Functional) appliance — still used today in both orthodontics and craniofacial orthopedics.
While Crozat’s work didn’t spread through Europe in the same way Andresen’s did, it showed that the U.S. was not only importing functional ideas but also generating its own.
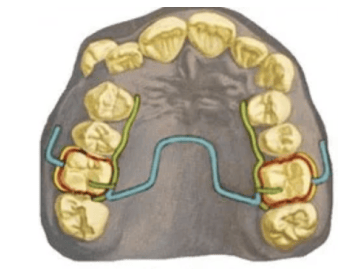
A removable device designed by George B Crozat. In: Spielman, AI. History of Orthodontics.

Crozat in situ. In:Crozat appliance. Orthodontics.
📍 Functional Appliance Timeline
1900s — Pierre Robin’s Monoblock (France)
1905 — Emil Herbst’s original Herbst appliance (Germany)
1919 — Crozat Appliance (USA)
1920s — Andresen-Häupl Activator (Denmark/Germany)
1930s — Korkhaus Activator refinements (Germany)
1920s–30s — Schwarz, Adams, Stockfisch, Tränkmann removable plates (Europe)
1950s — Wilhelm Balters’ Bionator (Germany)
1950s–60s — Rolf Fränkel Functional Regulators (East Germany)
Late 1970s — William Clark’s Twin Block (Scotland)
1979 — Hans Pancherz revives Herbst appliance (Germany)
1980s–Present — MARA, Jasper Jumper, Forsus, Carrière Motion (International)
1980s — Lingual Orthodontics refined (France, Germany → USA)
Today — ALF appliance (USA), blending Crozat principles with cranial orthopedics
📚 Sources & References
Primary Historical Sources
Robin, P. (1902). Sur la Respiration nasale et ses Malformations. Paris.
Andresen, V., & Häupl, K. (1936). Funktions-Kieferorthopädie. Leipzig: Thieme.
Herbst, E. (1934). Atlas und Grundriss der Kieferorthopädie. München: Lehmann.
Crozat, G.B. (1919). Technique for Orthodontic Correction without Extraction.
Balters, W. (1950). Der Bionator.
Fränkel, R. (1969). Regulation of Function in Orthodontics.
Clark, W.J. (1988). The Twin Block Technique.
Tweed, C.H. (1944). “The extraction of teeth in orthodontic procedure.” American Journal of Orthodontics and Oral Surgery, 30(8), 405–428.
Wiebrecht, A.T. (1930). Clinical Expansion Techniques with the Crozat Appliance.
Secondary & Contemporary References
Pancherz, H. (1979). “The Herbst appliance – its biologic effects and clinical use.” American Journal of Orthodontics, 76(4), 321–339.
Graber, L.W., Vanarsdall, R.L., Vig, K.W.L., & Huang, G.J. (2016). Orthodontics: Current Principles and Techniques. St. Louis: Elsevier.
Proffit, W.R., Fields, H.W., & Sarver, D.M. (2018). Contemporary Orthodontics. St. Louis: Elsevier.
Wahl, N. (2005). “Orthodontics in 3 millennia. Chapter 3: The rise of the specialists.” American Journal of Orthodontics and Dentofacial Orthopedics, 127(2), 307–315.
Spielman, AI. History of Orthodontics. In: Illustrated Encyclopedia of the History of Dentistry. 2024. https://historyofdentistryandmedicine.com/
Vaden, James L. A century of the edgewise appliance. doi:
10.4103/2321-1407.169949. https://apospublications.com/a-century-of-the-edgewise-appliance/
Brandt, Sidney. JPO Interviews Dr. Charles H. Tweed, Part 3. https://www.jco-online.com/archive/1968/02/81/
Pocket Dentistry. Contemporary fixed appliances. https://pocketdentistry.com/contemporary-fixed-appliances/
British Orthodontic Society. Functional-Appliances: Andresen Activator. https://bos.org.uk/museum-and-archive/appliances-and-equipment/functional-appliances/andresen-activator/
The activator and its modification - A review. Aameer Parkar1, Pavan Kumar Vibhute2, Chetan Patil3, Vinay Umale4*, Balagangadhar. https://ijodr.com/archive/volume/5/issue/2/article/4764/pdf
Bionator. https://de.slideshare.net/slideshow/bionator-258457198/258457198#5
Crozat appliance. Orthodontics. https://www.facebook.com/orthodontics.uk/photos/the-crozat-light-wire-appliance-for-okotoks-orthodontic-patients-wwworthotropics/486395294849755/
KFO Dr. Dr. Greuner. Herausnehmbare Zahnspangen. https://www.kfo-wittenberg.de/lose-zahnspange.html
Klasse II-Behandlung Erwachsener mithilfe der MALU-Apparatur. Dr. Jakub Malinowski und Katarzyna Jastrzębska. https://www.zwp-online.info/fachgebiete/kieferorthopaedie/funktions-kfocmd/klasse-ii-behandlung-erwachsener-mithilfe-der-malu-apparatur